The Evolution of Scientific Understanding of Laminitis: Historical Review from the 18th Century to Current Paradigms
- Horse Education Online

- 53 minutes ago
- 8 min read

Abstract
Equine laminitis is a debilitating and potentially fatal disorder of the hoof characterized by failure of the lamellar attachment apparatus. Although recognized for centuries under the term “founder,” scientific interpretations of its pathophysiology have undergone repeated paradigm shifts. Early descriptions emphasized vascular disturbance and systemic inflammatory triggers. Mid-twentieth-century advances focused on clinical standardization, most notably the Obel grading system. Late twentieth-century research reframed laminitis as a structural failure of the dermal–epidermal interface, highlighting basement membrane pathology and enzymatic degradation. In the twenty-first century, epidemiologic and experimental evidence led to the reclassification of laminitis as a clinical syndrome with distinct initiating pathways, including sepsis-associated, endocrinopathic, and supporting-limb forms.
This article presents a chronological review of the scientific understanding of laminitis through changing studies from the nineteenth century to the present, drawing exclusively from peer-reviewed literature. The historical path of laminitis in scientific thought illustrates how advances in pathology, molecular biology, and endocrinology reshaped the understanding of this complex disorder while preserving recognition of its multifactorial nature.
Many times, farriers must listen to lay people describe the causes for chronic laminitis (founder) and lack sufficient scientific information to counter false or outdated theories and scientific data.
Introduction
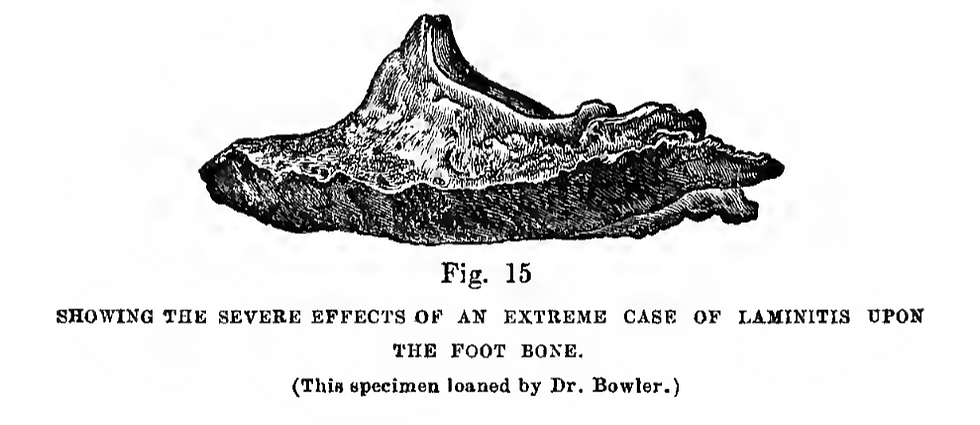
Laminitis is a painful condition of the equine digit involving disruption of the lamellar interface that suspends the distal phalanx within the hoof capsule. Clinically, it manifests as lameness, altered stance, increased digital pulses, and, in severe cases, displacement of the distal phalanx from the pull of the deep digital flexor tendon.
Despite centuries of recognition, its pathogenesis has remained controversial and evolving.
A historical review concisely summarized the persistent challenge:
“The history of laminitis has been a search for the cause or causes of laminitis and for effective treatment.”¹
This statement encapsulates the intellectual pathway of laminitis research. Over time, the disorder has been interpreted through successive physical processes alone: vascular compromise, inflammatory injury, basement membrane degradation, endocrine dysregulation, and biomechanical overload. The purpose of this review is to chronologically examine these conceptual transitions using peer-reviewed literature and historical analyses.
Historical Periods
The Beginning of Scientific Studies on Equines
Before veterinary medicine became a formal science, the role of the veterinarian as we know it today did not exist. Care of horses was largely the responsibility of farriers, whose work blended hoof care, basic medical treatment, and general animal management. Knowledge of disease and treatment was not standardized or scientifically tested. Instead, it was passed down through word of mouth, apprenticeships, and tradition. While many of these individuals were observant and genuinely committed to helping the animals in their care, their understanding was shaped by the broader medical beliefs of the time. These beliefs often included practices such as bloodletting and the use of topical mixtures based on humoral theory rather than evidence-based medicine. As a result, some treatments were ineffective or even harmful, despite being widely accepted. The historical material provided below offers a clear example of this, illustrating how conditions like founder were once treated using methods that reflect the limited scientific understanding of the period.

Nineteenth Century: Founder and the Vascular Hypothesis
In nineteenth-century veterinary medicine, laminitis was most commonly termed “founder.” Clinical descriptions emphasized heat in the feet, bounding digital pulses, reluctance to move, and the characteristic “sawhorse” stance. Overfeeding, grain overload, systemic illness, retained placenta, and excessive concussion, and changes in temperature were commonly cited precipitating factors.
The simple, predictable machine-like processes driven by physical forces was thought to create the condition, early authors consistently associated laminitis with disturbances in circulation. Congestion, inflammation, and altered perfusion of the foot were considered central to disease development. These vascular interpretations dominated professional discourse well into the twentieth century.
The vascular model provided a unifying explanation for diverse triggers, but did not account for the structural mechanics of lamellar failure until the end of the century.


Early to Mid-Twentieth Century: Clinical Standardization and Experimental Models
The twentieth century introduced systematic clinical classification. In 1948, Swedish veterinarian Nils Obel published a paper titled Studies on the histopathology of acute laminitis in which he described a grading system based on lameness severity and stance.
The Obel system enabled reproducible comparison across cases and experimental models. During this period, carbohydrate overload experiments became prominent in research settings, reinforcing inflammatory and vascular interpretations of laminitis pathogenesis.
Experimental induction of laminitis through oligofructose (sugar from prebiotic chicory root fiber) or grain overload supported the idea that systemic inflammatory mediators and circulatory disturbances contributed to lamellar damage. However, histologic mechanisms were not yet fully elucidated.
Late Twentieth Century: Lamellar Histopathology and Basement Membrane Pathology
Histopathology is the microscopic examination of biological tissue to study the manifestations of disease.
The late twentieth century marked a decisive shift toward structural pathology. Detailed histologic investigations focused on the dermal–epidermal interface, identifying early cellular changes in the lamellae.
Dr. Chris Pollitt described characteristic early lesions in experimentally induced laminitis:
“Earliest changes were rounding of the basal cell nuclei and elongation of secondary epidermal lamellae.”³

These findings reframed laminitis as a disease of lamellar structural integrity. Attention turned to basement membrane disruption, cytoskeletal alterations, and matrix metalloproteinase (MMP) activation. The concept of laminitis as primarily a basement membrane pathology gained prominence.
This mechanistic focus represented a departure from purely vascular explanations. Lamellar separation was interpreted as failure of cellular adhesion and extracellular matrix support, mediated in part by inflammatory signaling and enzymatic degradation.
Nevertheless, field cases increasingly revealed a lack of uniformity in cases. Not all naturally occurring laminitis resembled sepsis-associated experimental models, suggesting that multiple initiating mechanisms might converge on a shared structural endpoint.
Early Twenty-First Century: Recognition of Laminitis as a Clinical Syndrome
By the early twenty-first century, accumulating epidemiologic and mechanistic data led to reconsideration of laminitis as a single disease entity. A pivotal review articulated this paradigm shift:
“Laminitis is now considered to be a clinical syndrome associated with systemic disease or altered weight bearing rather than being a discrete disease entity.”⁴
This reframing acknowledged that laminitis can arise from distinct initiating contexts, including:
Sepsis or systemic inflammatory response syndrome
Endocrine disorders such as equine metabolic syndrome and pituitary pars intermedia dysfunction
Altered weight bearing in supporting-limb laminitis
Importantly, endocrine-associated laminitis emerged as highly prevalent:
“Laminitis associated with endocrine disease… is now believed to be the predominant form…”⁴
The endocrine system is a network of glands that produce and release hormones directly into the bloodstream to regulate vital bodily functions, including metabolism, growth, mood, and reproduction. It acts as a chemical messenger system, with key glands such as the pituitary, thyroid, adrenals, and pancreas influencing almost every cell and organ in the body.
This observation required reinterpretation of decades of experimental data derived largely from sepsis models.
The Endocrine Paradigm: Hyperinsulinemia and Cellular Distortion
The recognition of hyperinsulinemia as a causal factor in laminitis transformed the field. Experimental studies demonstrated that sustained high insulin concentrations alone can induce laminitis without overt systemic inflammation. Hyperinsulinemia leaves glucose circulating in the blood. Because glucose levels do not drop, the pancreas continues to discharge insulin, leading to elevated concentrations of insulin in the bloodstream.

The implications for structural pathology were significant. The 2018 review noted:
“The designation of laminitis as a primary and severe basement membrane pathology now requires revision.”⁴
Instead of early basement membrane destruction, endocrinopathic laminitis is characterized by cellular stretching and morphological distortion:
“…stretching and elongation of the lamellar cells [is] an early and key event…”⁴
This shift redirected attention toward insulin signaling pathways, growth factor receptor activation, and cytoskeletal dynamics within lamellar epithelial cells.
Supporting-Limb Laminitis: Biomechanics and Local Perfusion
Supporting-limb laminitis further broadened the syndrome framework. In these cases, excessive weight bearing on a contralateral limb leads to lamellar failure. Unlike endocrine or sepsis-associated forms, the initiating factor is mechanical overload with associated perfusion mismatch and metabolic stress.
Perfusion is the essential, continuous process of delivering oxygenated blood through the vascular system to tissues and organs.
The inclusion of supporting-limb laminitis within the broader syndrome emphasizes convergence on a final common pathway: disruption of lamellar attachment and mechanical destabilization of the distal phalanx.

Discussion
The scientific evolution of laminitis concepts illustrates cumulative refinement rather than simple replacement of theories. Vascular disturbance remains relevant in sepsis-associated disease. Basement membrane integrity remains critical to structural stability. Endocrine signaling pathways are central in many contemporary cases. Biomechanical stress is clearly pathogenic in supporting-limb scenarios.
The historical trajectory reflects advances in scientific methodology. Gross pathology and clinical observation characterized early periods. Histologic and molecular techniques reshaped late twentieth-century interpretations. Endocrinology and metabolic research dominate contemporary inquiry.
Importantly, laminitis research has progressively embraced the state of being diverse. The syndrome framework reconciles divergent initiating mechanisms while recognizing a shared structural endpoint. As summarized in modern review literature:
“Understanding of laminitis continues to evolve as research identifies distinct initiating causes and mechanisms.”⁴
This evolution mirrors broader developments in comparative pathology, where multifactorial syndromes replace monolithic disease constructs.

Conclusion
From nineteenth-century descriptions of founder to twenty-first-century molecular and endocrine paradigms, scientific understanding of equine laminitis has undergone repeated transformation. Early vascular theories gave way to structural and enzymatic models, which were subsequently integrated into a broader syndromic framework incorporating endocrine and biomechanical pathways.
Despite substantial progress, laminitis remains incompletely understood and continues to pose significant welfare and economic challenges. The enduring relevance of the historical observation remains clear:
“The history of laminitis has been a search for the cause or causes of laminitis and for effective treatment.”¹
Future advances will likely depend on continued integration of endocrinology, biomechanics, molecular signaling, and translational pathology within a unified but flexible conceptual model. It is probable that there may be multiple pathways that lead to the same end result, laminitis, which would create a variety of farrier options for the treatment of this insidious disease.
References
Heymering HW. A historical perspective of laminitis. Vet Clin North Am Equine Pract. 2010;26(1):1–11.
Meier AD, de Laat MA, Reiche DB, et al. A modified Obel method for the severity scoring of endocrinopathic equine laminitis. PeerJ. 2019;7:e7084.
Pollitt CC. Basement membrane pathology: a feature of acute equine laminitis. Equine Vet J. 1996;28(1):38–44.
Patterson-Kane JC, Karikoski NP, McGowan CM. Paradigm shifts in understanding equine laminitis. Vet J. 2018;231:33–40.










Comments