Splint Bone Injuries, an Advanced Overview
- Horse Education Online

- Jan 22
- 7 min read
Updated: Feb 13

Anatomical Overview
The splint bones are located on the palmar aspect of the cannon bone (metacarpus) in the fore limbs, and the plantar aspect of the cannon bone (metatarsus) in the hind limbs. The cannon bone, or third metacarpal bone, is the primary weight-bearing structure of the distal limb of the horse. Splint bones are considered vestigial, meaning they are underdeveloped remnants of what were once fully weight-bearing digits in the horse’s evolutionary ancestors. Anatomically, they are identified as the second and fourth metacarpal or metatarsal bones, which flank the centrally positioned cannon bone.
Forelimb Anatomy
The medial splint bone is also called the second metacarpal bone. It lies on the inside of the limb and is clinically the most commonly affected splint bone due to biomechanical loading and interference.
Medial splint bones are under greater biomechanical stress as they lie closer to the centerline of the body, and therefore bear greater weight. For this reason, the head of the medial splint bones has two facets to better support the carpal bones.

Medial splint bones are additionally at greater risk of traumatic injury from the horse striking itself with the opposing limb or hoof. Learn more about interfering, the gait fault that most commonly leads to splints, here.
The lateral splint bone is the fourth metacarpal bone and lies on the outside of the limb, where it is more susceptible to external trauma. Its head is one-faceted.
Hindlimb Anatomy
The medial splint bone in the hind limb is the second metatarsal bone, positioned on the inside of the hind limb. Just like in the forelimb, the medial splint bone is under greater biomechanical stress, and therefore has a two-faceted head to support the tarsal bones.
The lateral splint bone is the fourth metatarsal bone, located on the outside of the limb. It's head is one-faceted.
The splint bones taper progressively as they extend distally from the carpal or tarsal joint. Near their distal ends, they form a palpable bony enlargement, commonly referred to as a “button” or nodule, located several centimeters proximal to the fetlock joint. Throughout their length, the splint bones run parallel to the cannon bone, contributing to the longitudinal stability of the limb.
Ligamentous and Fascial Attachments
Splint bones are attached to the cannon bone via the interosseous ligament, a fibrous structure that provides both support and limited mobility. In young horses, this ligament allows a small degree of motion between the splint and cannon bones, which is thought to help dissipate concussive forces during locomotion.
The interosseous ligament varies considerably between individual horses in terms of thickness and elasticity. With age and continued mechanical stress, this ligament typically undergoes progressive ossification, reducing mobility between the bones.
In some older horses, partial or complete fusion of the splint bone to the cannon bone may occur. While often clinically insignificant, this fusion reflects long-term adaptation to repetitive stress.
A dense layer of fascia overlies the tendons in the proximal metacarpal and metatarsal regions and attaches directly to the splint bones. Fascia is a critical connective tissue system that wraps, supports, and separates muscles, bones, and organs, while also contributing to force transmission, coordinated movement, and sensory feedback.
A band-like structure extends distally from the end of each splint bone toward the proximal sesamoid bones, further integrating the splint bones into the suspensory apparatus of the distal limb.
Articulations
The heads of the splint bones serve as a structural platform for the lower row of carpal or tarsal bones, contributing to joint stability. As previously discussed, medial splint bones have a two-faceted head, while lateral splint bones have a one-faceted head. This is to account for the additional stress placed on the medial splint bone as it lies closer to the centerline of the body.
The medial splint bone forms a full articulation with the second carpal bone (C2) in the forelimb and the second tarsal bone (T2) in the hindlimb. This complete articulation explains why pathology of the medial splint bone may be associated with adjacent joint discomfort. Download our Tarsus and Carpus flashcards to study tarsal and carpal anatomy in depth.
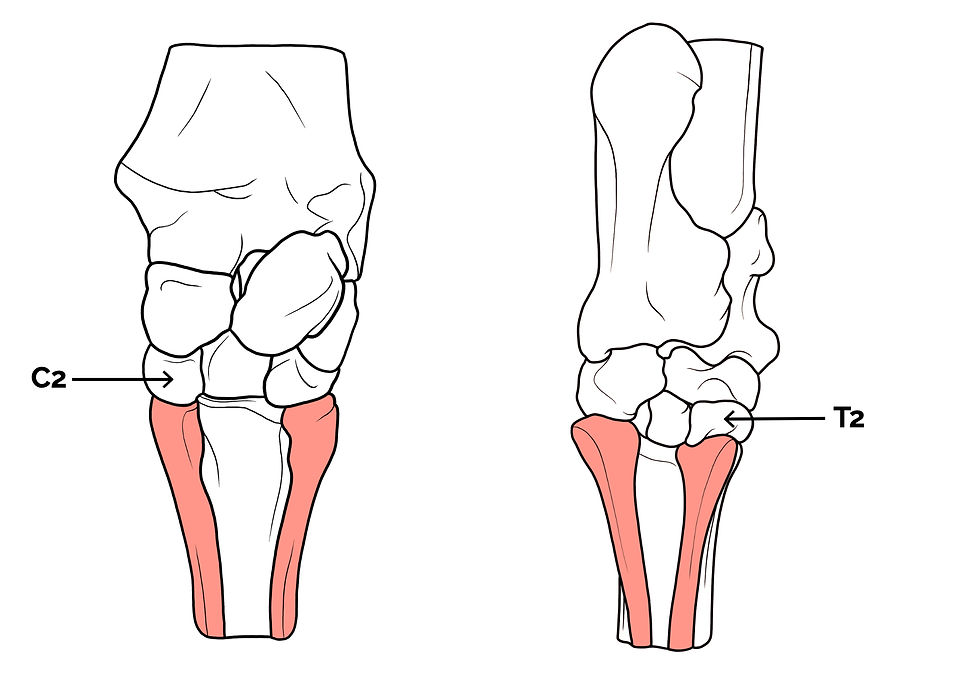
The splint bones in relation to the carpal and tarsal bones (palmar/plantar view) The lateral splint bone supports only half of the fourth carpal bone, making it less involved in weight-bearing but more vulnerable to trauma.
Classification of "Splints"
A splint is defined as a bony enlargement (exostosis) involving the second or fourth metacarpal or metatarsal bones. An exostosis is a benign proliferation of bone that develops in response to stress, inflammation, or trauma.
Three primary types of splints are recognized:
Intermetacarpal / Intermetatarsal Splint
This form involves an exostosis developing between the cannon bone and a splint bone. It is commonly associated with injury or inflammation of the interosseous ligament and represents the most frequently encountered splint type in clinical practice.

Intermetacarpal / Intermetatarsal splint Postmetacarpal / Postmetatarsal Splint
This splint occurs on the palmar or plantar (axial) surface of a splint bone. Its location may place it closer to important soft tissue structures, increasing the potential for clinical significance.

Postmetacarpal / Postmetatarsal splint Blind Splint
A blind splint is an exostosis on the axial (central) surface of a splint bone that cannot be detected by palpation and is not visible on standard radiographs. These splints may still cause lameness, particularly if they impinge on the suspensory ligament.

Blind Splint
Green Splints
The term “green splint” refers to an actively forming splint characterized by heat, swelling, and pain on palpation.
At this stage, inflammation is still present, and bone remodeling is ongoing.
Most green splints produce a mild Grade 3 lameness when the horse is trotted on a firm surface in a small circle.
Once inflammation resolves and pain is no longer present, the splint is considered “set” and is no longer classified as a green splint.
Radiographic examination is essential to:
Determine the size and exact location of the splint
Identify any associated fractures of the splint bone
Etiology
Interosseous Ligament Injury
Tearing or inflammation of the medial interosseous ligament commonly occurs when horses are first placed into structured work.
The ligament is not yet conditioned to repetitive loading, making it particularly vulnerable during early training.
Physical Trauma
Young horses frequently strike the medial splint bone with the opposing limb while playing, leading to localized inflammation or tearing.
Lateral splint bones are more susceptible to trauma from external sources such as other horses or solid objects.
Medial splint bones are most often injured by interference from the contralateral limb.
Conformation-Related Stress
Conformational abnormalities such as base-narrow stance, toed-out feet, angular limb deformities, and offset knees increase mechanical strain on the medial splint bone.
These conformations promote inward limb motion and increase stress on the medial interosseous ligament.
Training Factors
Excessive work in tight circles, particularly in young horses, concentrates force on the medial splint bone.
Repetitive strain can lead to ligament tearing followed by reactive bone formation as part of the healing process.
Diagnosis
Splints are diagnosed through a combination of clinical examination, lameness evaluation, and diagnostic imaging, with the goal of confirming the presence of a splint, determining its stage of development, and identifying any associated complications.
Diagnosis begins with a thorough physical examination of the limb. Palpation of the splint bones may reveal localized heat, swelling, or pain, particularly in cases of green splints. Firm, non-painful bony enlargements suggest a set splint. Careful comparison with the contralateral limb is essential, as mild splints may be subtle.

Diagnostic imaging, particularly radiography, is central to definitive diagnosis. Radiographs allow visualization of bony proliferation, assessment of the splint’s size and location, and identification of splint bone fractures. Imaging is especially important when lameness is disproportionate to palpable findings or when a blind splint is suspected.


Treatment
Conservative Management
Rest for several weeks is the most effective treatment and allows inflammation to resolve and bone remodeling to stabilize.
After the acute phase, light exercise on soft footing may promote controlled healing.
Counter-irritants are not recommended, as they increase inflammation, disrupt orderly bone formation, and may prolong recovery time.
Surgical Intervention
Splint bone fractures, particularly those involving the distal one-third, are most appropriately treated surgically.
Surgical removal of splint bone enlargements in show horses often yields poor outcomes, as surgery may stimulate additional bone formation.
Approximately 50% of these procedures are considered successful.
Prognosis
In cases that do not involve blind splints impinging on the suspensory ligament or high splint bone fractures, the prognosis is excellent.
Pain typically resolves rapidly, although the bony enlargement may persist as a cosmetic blemish.
Over time, gradual bone remodeling may occur, and the splint may become minimally noticeable or clinically insignificant.
FAQ: Splint Bone Injuries
1) Where are the splint bones located in the horse’s limb?
Splint bones run alongside the cannon bone: on the palmar aspect in the forelimbs and the plantar aspect in the hindlimbs. They are the 2nd and 4th metacarpal or metatarsal bones that flank the cannon bone.
2) Which splint bone is injured most often, and why?
The medial splint bone is most commonly affected because it sits closer to the horse’s centerline, experiences greater biomechanical loading, and is also a common target for interference from the opposite limb.
3) What is the “button” people feel near the fetlock?
Splint bones taper as they go down the limb and can form a palpable enlargement several centimeters above the fetlock, often called a “button” or nodule.
4) What connects the splint bones to the cannon bone?
They’re attached via the interosseous ligament, which provides support and limited mobility. In young horses it allows small motion (helpful for dissipating force), and it often ossifies with age, sometimes partially fusing the splint to the cannon bone.
5) What are the main types of “splints” (exostosis)?
The article describes three primary types:
Intermetacarpal / intermetatarsal splint (between the cannon and splint bone; most common)
Postmetacarpal / postmetatarsal splint (on the palmar or plantar surface of a splint bone)
Blind splint (axial surface, not palpable and may not show on standard radiographs; can still cause lameness if it impinges the suspensory ligament)
6) What is a “green splint”?
A green splint is an actively forming splint with heat, swelling, and pain on palpation, where inflammation and bone remodelling are still ongoing.
7) What are the most common causes of splint bone injuries?
The post highlights several contributors, especially in young horses starting work:
Interosseous ligament strain/tearing
Physical trauma (interference medially; external trauma laterally)
Conformation-related stress (base narrow, toed out, angular limb deformities, offset knees)
Training factors (excessive tight circles, repetitive strain)
8) How are splints diagnosed and treated?
Diagnosis combines exam and lameness evaluation with radiographs to confirm size/location and rule out fractures; imaging is especially important when lameness doesn’t match palpation or when a blind splint is suspected. Treatment is typically rest for several weeks; light controlled exercise on soft footing may be used after the acute phase.
Counter irritants are not recommended, and surgery is most appropriate for certain splint bone fractures (especially distal one third), while removing splint enlargements for cosmetic reasons has mixed success.










Comments